You feel it before you see it. That sharp click deep in your groin when you squat. A sudden catch that locks up mid-stride. For athletes, these symptoms often signal a Hip Labral Tear is damage to the fibrocartilaginous rim lining the acetabular socket of the hip joint. Sports requiring repetitive rotation-think basketball pivots, soccer turns, or football cuts-stress this rim until it gives way. While we didn't fully understand these injuries in the 90s, modern orthopedics has identified them as a leading cause of hip dysfunction in active individuals.
The stakes are high. Ignoring a torn labrum isn't just about pain; it accelerates wear and tear on the joint surface. Untreated tears carry a 4.5 times higher risk of developing osteoarthritis within a decade. This article breaks down the path from that initial nagging sensation to recovery, focusing on why standard MRIs often miss the mark and why arthroscopy has become the gold standard for many competitive athletes.
Anatomy and Causes of Hip Labral Tears
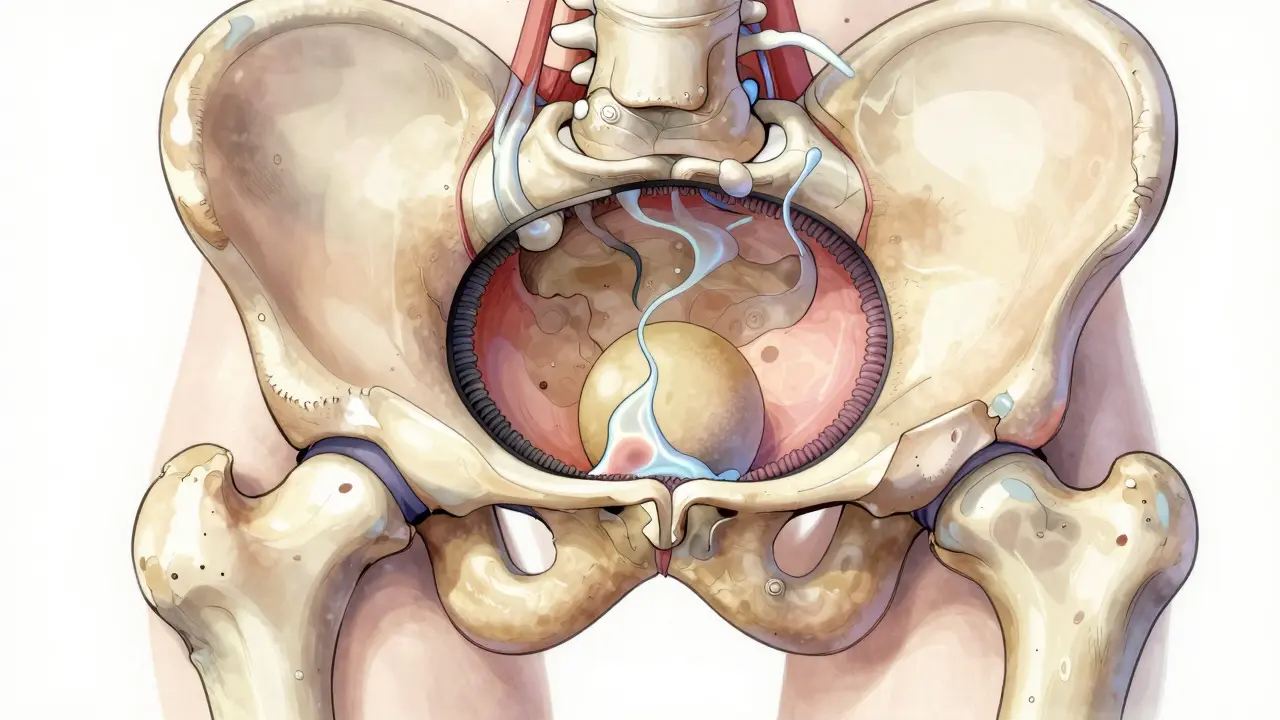
To fix the hip, you need to understand the machine. The acetabulum acts like a bowl, holding the ball of the femur in place. The labrum is the gasket lining that bowl. It creates suction, keeps fluid inside to cushion the bone, and distributes load. When that gasket tears, pressure escapes. Instability sets in.
In most athletes, the damage stems from Femoroacetabular Impingement (FAI) is a bony deformity where the femoral head pinches the labrum during movement. Think of a door hinge that rubs against the frame every time you open it. Over time, the rubber seal wears out. Research indicates that roughly 35-50% of elite athletes under 40 with chronic hip pain have this pathology. While dysplasia-a shallow hip socket-is less common, it presents a unique challenge where the ball sits loosely, forcing the labrum to work overtime to hold stability.
The Diagnostic Challenge: Why Standard MRIs Fail
If you walk into a generic clinic, they will likely order a standard MRI. Here is the hard truth: conventional MRIs detect labral tears only 35% to 60% of the time. The soft tissue contrast simply isn't sensitive enough to show small partial-thickness tears.
The diagnostic test of choice is Magnetic Resonance Arthrography (MRA) is an MRI scan involving the injection of contrast dye directly into the joint space. This dye fills the cracks in the labrum like water filling a fissure in a dam. Sensitivity jumps to 90-95%. Before any imaging, however, the physical exam matters. Doctors use the FADIR test (flexion, adduction, internal rotation) to reproduce pain. If you cannot replicate the exact moment of locking without manual manipulation, imaging is even more critical.
| Modality | Sensitivity for Labral Tears | Clinical Utility |
|---|---|---|
| X-Ray (AP/Lateral) | <5% (indirect signs only) | Rules out fractures, shows FAI morphology/dysplasia |
| Standard MRI | 35-60% | Evaluates muscles, tendons, avascular necrosis |
| MRI Arthrogram (MRA) | 90-95% | Gold standard non-invasive imaging for the labrum |
Treatment Protocols: Conservative First?
Before booking surgery, almost all protocols mandate a trial of conservative management. This usually involves 4-6 weeks of relative rest and NSAIDs is non-steroidal anti-inflammatory drugs like ibuprofen or naproxen sodium. These reduce inflammation that clouds judgment during rehabilitation. About 30% to 40% of athletes achieve complete symptom resolution this way. Another 35% find temporary relief with corticosteroid injections, though these are diagnostic tools as much as treatments-if the steroid kills the pain completely, you've confirmed the source.
Physical therapy is controversial. Some argue the labrum can't be "strengthened" back to health once torn, while others contend core stability reduces shear forces on the joint. Specialized sports programs report up to 65% success avoiding surgery through targeted load management. However, if pain persists after three to six months, delaying intervention risks turning a single labral tear into cartilage delamination.
Hip Arthroscopy: Procedure and Repair Techniques
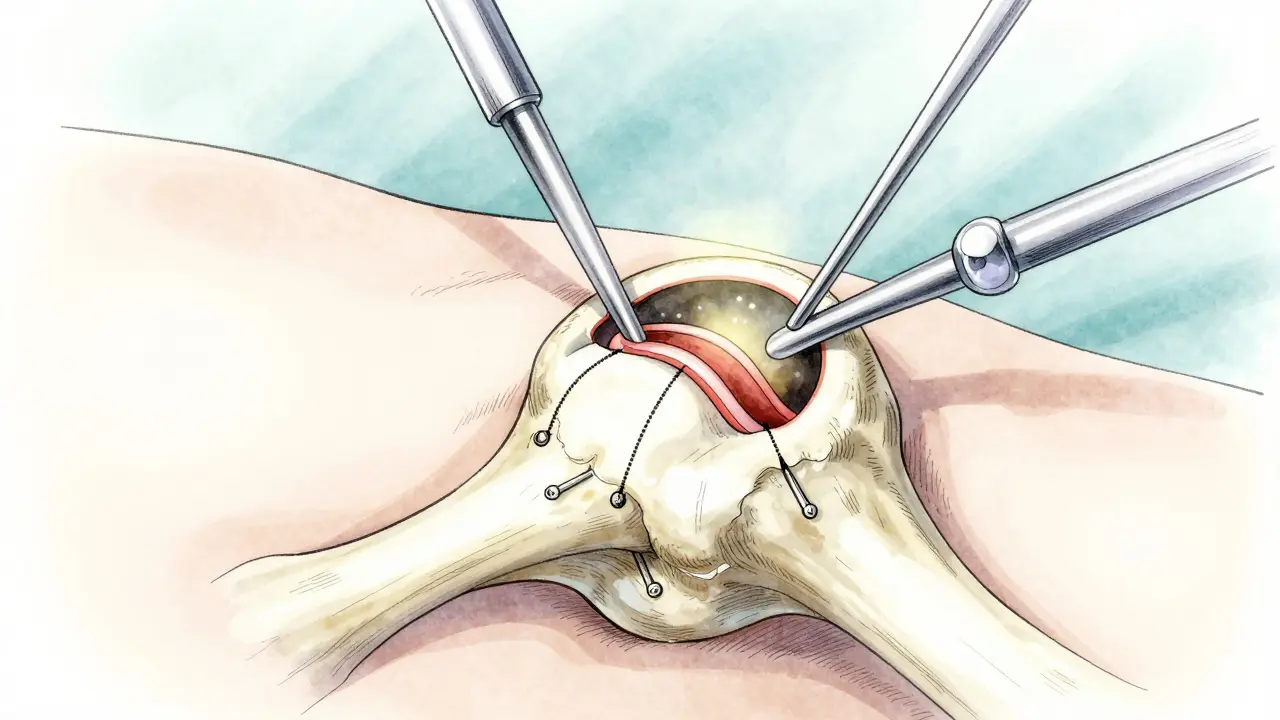
When conservative care fails, Hip Arthroscopy is a minimally invasive surgical procedure using a camera and instruments inserted through small portals. is the definitive treatment. Unlike knee scopes, hip scopes require significant surgeon expertise due to the complex geometry. You need 50 to 100 supervised cases to master the portal placement safely.
There are two primary outcomes during the procedure. Debridement simply cleans up frayed tissue. It is faster and easier but carries a higher re-tear rate. Labral repair, conversely, involves sewing the tissue back to the bone using suture anchors. In 2023, the FDA approved the first bioabsorbable anchor system (BioX) designed specifically for this. Traditional metal or PEEK anchors remain widely used, offering robust fixation. Choosing a surgeon who performs primarily repairs over debridements is crucial; repair preserves the suction seal, lowering arthritis risk long term.
Rehabilitation Timelines and Return to Play
Patience is the hardest part of recovery. After a repair, you cannot just walk away from crutches the next day. The timeline splits into phases. Weeks one to six focus on protection. You might be weight-bearing limited to prevent strain on the suture anchors. By week 12, strength training ramps up. By month six, you aim for full functional testing.
Metric-based clearance is vital. Simply being pain-free isn't enough. Surgeons require quadriceps strength symmetry exceeding 90% compared to the uninjured leg. Hip internal rotation must reach 30 degrees pain-free. If you skip to running too early, say at week eight, you risk anchor pull-through. Studies show 85-90% of competitive athletes return to their pre-injury level following arthroscopic repair, provided they respect the healing window.
Risks, Complications, and Long-Term Outlook
Every surgery carries risks. Nerve injury occurs in about 1-2% of cases, sometimes resulting in numbness near the portals. Heterotopic ossification, where bone forms in soft tissue, happens in 5-10% of patients. Persistent pain affects roughly 15-20% despite successful repair. Revision surgery rates sit around 8-12% over five years. These numbers drop significantly when underlying issues like dysplasia are addressed concurrently. If you have a shallow socket, repairing the labrum alone leads to failure 65% of the time. A comprehensive structural correction is mandatory in those anatomies.
Looking ahead, the industry is shifting toward regenerative options. Platelet-rich plasma (PRP) injections show promise, helping 55% of patients avoid surgery entirely at the 12-month mark. As 3D planning software integrates with surgical navigation, precision continues to improve. But for now, the combination of accurate MRA diagnosis and skilled arthroscopic repair remains the best pathway to keeping athletes moving.
Frequently Asked Questions
Can a hip labral tear heal on its own without surgery?
Yes, approximately 30-40% of athletes can manage symptoms successfully with conservative care alone. This typically involves relative rest, anti-inflammatories, and specialized physical therapy. However, larger tears or those causing mechanical locking often require surgical intervention.
How long does it take to recover from hip arthroscopy?
Recovery depends on the procedure type. If only debridement was done, return takes 3-4 months. For labral repair with suture anchors, the timeline extends to 5-6 months to ensure the tissue heals securely to the bone.
Is an MRA better than a standard MRI for diagnosing hip tears?
Yes. Standard MRIs miss up to 65% of labral tears. MRA involves injecting contrast dye into the joint, which highlights tears with 90-95% sensitivity, making it the preferred diagnostic tool before surgery.
Does hip surgery increase the risk of future arthritis?
Untreated tears carry a much higher risk of arthritis. Properly executed labral repair aims to preserve joint function. However, if the tear causes severe cartilage damage before treatment, arthritis progression may still occur regardless of surgery.
What are the warning signs of a re-tear after surgery?
Symptoms returning to baseline intensity, new episodes of clicking or catching, and increased instability during pivoting motions are red flags. Persistent pain beyond the expected recovery timeline warrants follow-up imaging.
Hip problems are always suspicious when companies push MRI deals 🤨. They want your money more than your health honestly. Seems like they hide the cheaper solutions on purpose. Standard scans fail way too much for comfort. We are just pawns in their billing game system. Don't trust the initial diagnosis blindly ever. 😉
I hope you are taking care of yourself regardless of what anyone says. Health comes first for us all in the long run. Ignoring pain signals usually leads to bigger issues later on. Please listen to your body and get checked properly. 😊💕
The statistics regarding sensitivity rates are absolutely crucial for everyone! ! ! Why does this fact get ignored so often?!!!! Conventional MRIs simply do not detect the pathology correctly!!! We need more funding for arthrograms everywhere!!! The delay causes permanent damage!!! Do not wait until it hurts!!!
First things first we really need to acknowledge the importance of early detection here. It saves so much pain down the road. People ignore their symptoms until it is too late for simple fixes. The labrum acts as a seal for the hip joint after all. Without it everything falls apart quite quickly. You might feel like you are fine but your body knows better. This article does a great job explaining the imaging issues. Standard scans really miss the small tears often enough. That leads to people getting bad advice from clinics. We need more awareness about magnetic resonance arthrography specifically. Doctors should know this test is superior for diagnosis. Athletes deserve the best care without hesitation. Recovery takes patience but results are worth the wait. Keep pushing forward with your health journey always. Stay strong through the rehabilitation process.
The anatomy explanation was clear and helpful for me today. Understanding the mechanics behind impingement changes how you move. Many athletes benefit from early screening protocols now. Prevention remains the best strategy for longevity in sport. Take care of your hips consistently.
I am so happy to see this kind of information shared!!! Everyone needs to learn about these signs!!! Pain should never be ignored!!! It is important to advocate for your own health!!! Get the right tests done ASAP!!! Hope you all recover quickly!!! 💪😊✨
impingement mechanics are complex and FAI is rarely diagnosed correctly. surgeons push for scopes to bill codes not cure patients. contrast dye has risks ignored by standard protocols. FADIR test reliability is low sensitivity. clinical correlation matters more than radiology images.
Thanks for bringing up the diagnostic limitations 🙏 It is good to be informed about the options. Listening to specialists who understand biomechanics helps immensely. 👍
Pain whispers before it screams loudly in the soul. Our bodies are temples holding deep secrets. When the gasket breaks the flow of life gets blocked. Art and science meet on the operating table. Healing is a journey of the spirit and bone. Colors fade when the hip clicks wrong.
I think the philosophical view on pain management adds a lot to the conversation. Understanding why we hurt helps us heal faster mentally. It creates a bridge between physical injury and recovery mindset. Your perspective on the human experience is valuable here. Thanks for sharing such thoughtful insights.
You people are lazy for waiting so long to get proper testing done. Basic diligence should mean seeking advanced imaging immediately. Ignoring the osteoarthritis risk is irresponsible behavior. Medical professionals are trying to help not harm you. Stop making excuses for ignoring obvious physical decline.
We need to hold ourselves accountable for our health choices 😠 Ignoring warnings is not okay for anyone. Please get the scan that actually works. 🚫❌
Athletic performance relies heavily on joint integrity and stability mechanisms. Kinetic chains break when proximal structures fail like the acetabular labrum. Rehabilitation protocols must address femoroacetabular motion specifically. Return to play criteria should include functional imaging confirmation. Biomechanical analysis prevents recurrence significantly.
The systemic failure of primary diagnostics reveals deeper industry rot. Imaging artifacts mask reality while profit margins stay green. Patients get lost in the bureaucratic noise. We analyze the chaos but the outcome remains static. Data points scatter without direction or hope.
Solid read 👌